Definition
Azotemia refers to an increase in blood concentrations of non-protein nitrogen compounds, primarily urea and creatinine. These substances are waste products from protein metabolism and are normally eliminated by the kidneys. Azotemia thus reflects a disruption in renal function or changes in renal blood flow. It is measured through laboratory tests and serves as an indirect indicator of kidney failure. Depending on values and clinical context, it can be classified as prerenal, renal, or postrenal azotemia. This classification depends on the underlying cause, whether it is reduced renal perfusion, direct kidney tissue damage, or urinary tract obstruction. Azotemia alone does not provide a precise diagnosis but triggers additional investigations to identify the exact origin of kidney dysfunction. It is frequently monitored in patients with cardiovascular, hepatic, or chronic kidney diseases.
Origin and Context of Use
The term azotemia combines “azote” (nitrogen) and “-emia” (presence in blood). Its clinical use dates back to the early 20th century with the standardization of urine and blood analyses. Today, azotemia is evaluated in routine laboratory workups when risk factors for kidney dysfunction are present: hypertension, diabetes, dehydration, or use of nephrotoxic medications. It is also used in hospital settings to monitor critically ill patients or those under intensive therapy. Azotemia guides medical decision-making, particularly regarding medication dose adjustments or initiation of renal replacement therapy.
How Does It Work?
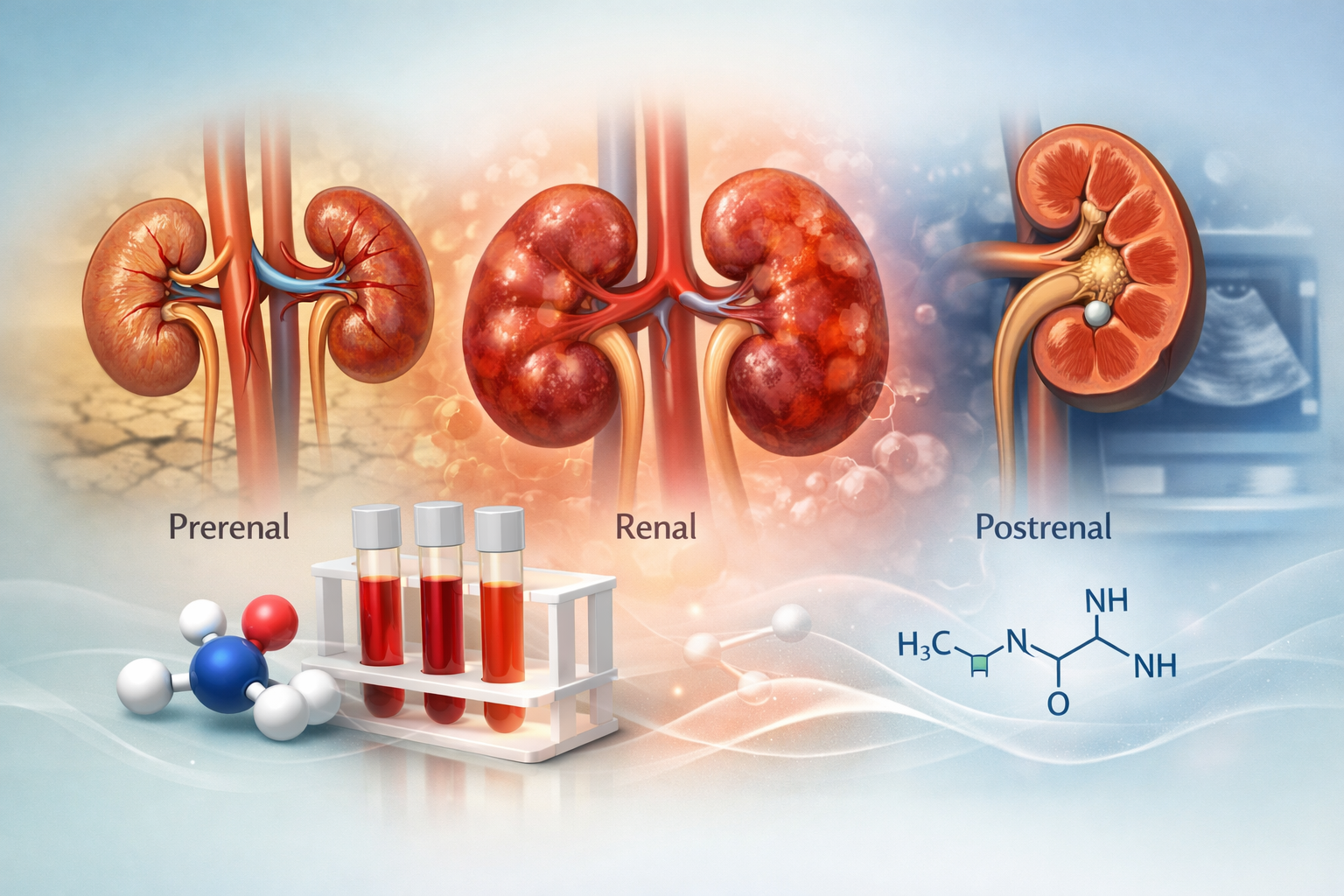
Azotemia results from an imbalance between the production and excretion of nitrogenous waste. Dietary proteins are broken down into amino acids, whose catabolism releases ammonia, which is then converted to urea in the liver via the urea cycle. Creatinine, derived from muscle metabolism, is also excreted by the kidneys. When glomerular filtration is insufficient or renal blood flow decreases, these wastes accumulate in the blood, leading to azotemia. Three types are distinguished: prerenal, caused by reduced renal perfusion (dehydration, heart failure); renal, due to direct renal parenchymal damage (acute nephropathy, glomerulonephritis); postrenal, secondary to urinary tract obstruction (stones, tumors, prostatic hypertrophy). Laboratory measurement of urea and creatinine, along with the urea/creatinine ratio, helps differentiate these forms. Complementary tests such as renal ultrasound or CT scan are sometimes necessary to identify obstruction or structural damage.
When Is It Used?
Azotemia is monitored in cases of:
-
chronic and acute kidney disease follow-up;
-
preoperative assessments to evaluate kidney function before anesthesia;
-
monitoring dehydrated patients or those in hypovolemic shock;
-
controlling the effect of nephrotoxic drugs, such as non-steroidal anti-inflammatory drugs or ACE inhibitors;
-
assessing patients with suspected urinary obstruction, like stones or prostatic hypertrophy.
Benefits and Objectives
Evaluating azotemia allows:
-
✓ early detection of kidney dysfunction before symptoms appear;
-
✓ guidance on the type of renal lesion (prerenal, renal, postrenal);
-
✓ adjustment of doses of renally excreted medications;
-
✓ monitoring the effectiveness of renal replacement therapy;
-
✓ prevention of metabolic complications such as acidosis or hyperkalemia.
Risks, Limitations or Controversies
Azotemia does not always indicate the severity of kidney damage. Values can be influenced by hydration, protein intake, or muscle mass. Isolated urea elevation can occur after a high-protein diet or fasting without kidney impairment. Azotemia alone does not always clearly differentiate prerenal and renal causes without additional tests. In elderly or malnourished patients, creatinine may remain normal despite significant glomerular filtration impairment. Relying solely on these markers may delay detection of early kidney failure.
Research and Innovations
Research focuses on early detection of kidney dysfunction using more sensitive biomarkers, such as cystatin C or urinary NGAL. Models combining azotemia, creatinine, and automated renal imaging are being tested to improve differential diagnosis of prerenal and renal forms. Continuous monitoring techniques, such as wearable sensors measuring blood nitrogen markers, are being explored for high-risk patients. Artificial intelligence is used to correlate azotemia with other physiological parameters to predict kidney failure progression and personalize treatment.
Short FAQ
What is azotemia? Azotemia is the increase of urea and creatinine in the blood, indicating impaired kidney function.
What are the types of azotemia? Prerenal, renal, or postrenal, depending on the cause of dysfunction.
How is azotemia measured? By blood tests measuring urea and creatinine.
Is azotemia always pathological? No, it may vary with diet, dehydration, or muscle mass.
What symptoms appear? Fatigue, nausea, or confusion mostly occur in advanced kidney failure.
Can azotemia be prevented? By maintaining proper hydration and monitoring chronic kidney disease.
Does azotemia guide treatment? Yes, it helps adjust medications and determine renal replacement therapy.
Are other tests needed? Often, ultrasound or CT scans are required to detect obstruction or lesions.
Is chronic azotemia dangerous? It indicates an increased risk of kidney failure and requires regular follow-up.
What is the relation with creatinine? Creatinine complements azotemia to assess glomerular filtration and differentiate causes.
Scientific context
Field: Clinical medicine, biology, and preventive health
Biological process: Human physiology, pathology, and health-related mechanisms
Related systems: Metabolic, immune, cardiovascular, nervous, and cellular systems
Relevance to longevity: Understanding medical terminology and biological processes helps clarify how diseases, symptoms, biomarkers, and treatments influence long-term health, prevention, and healthy aging.
Key Takeaways
Azotemia reflects the accumulation of urea and creatinine in the blood. It indicates impaired kidney function, whether prerenal, renal, or postrenal. Measuring it enables early diagnosis, therapeutic monitoring, and adjustment of nephrotoxic treatments, but interpretation must consider the clinical context.
Related Longevity Concepts