Definition
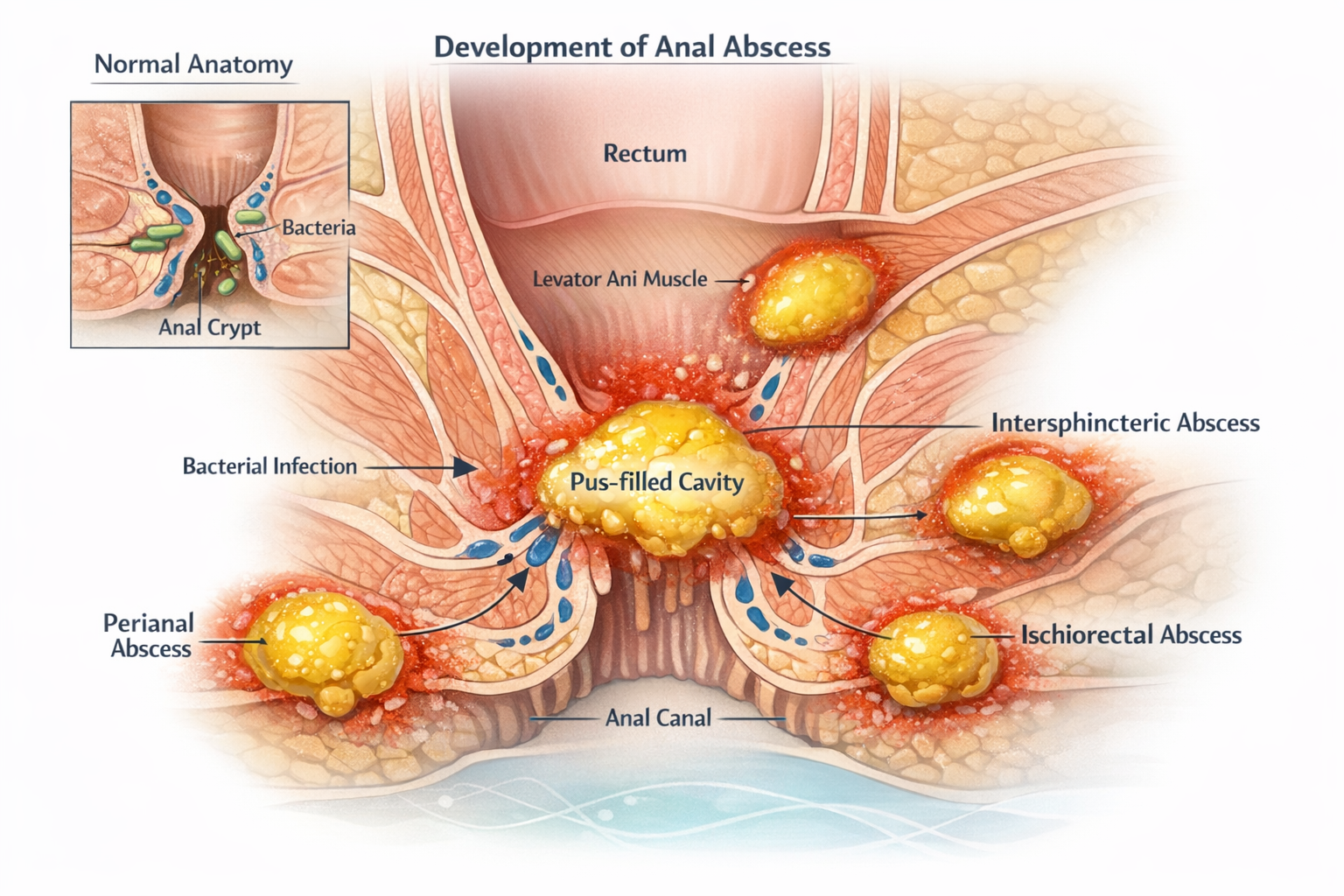
An anal abscess is a localized collection of pus in the tissues surrounding the anus or rectum. It usually results from a bacterial infection of an anal gland, called a cryptoglandular gland. When the gland’s drainage canal becomes blocked, intestinal bacteria multiply in the surrounding tissues, causing inflammation and forming a pus-filled cavity.
Abscesses can develop in various areas around the anus. The most common are perianal abscesses, located just under the skin around the anal opening. Other deeper locations include ischiorectal, intersphincteric, or pelvirectal abscesses.
The main symptom is severe anal pain, often throbbing, associated with a red, swollen, and warm area near the anus. Fever, general fatigue, or purulent discharge may also occur.
This is an acute infection that requires prompt medical attention. Without treatment, the abscess can spread to neighboring tissues or develop into an anal fistula, a channel connecting the skin to the inside of the anal canal.
Origin and context of use
Descriptions of anorectal infections date back to ancient medical texts. Physicians like Hippocrates already observed pus collections around the anus and their fistulous complications. Modern understanding of anal abscess mechanisms developed in the 20th century through colorectal surgery research.
Today, anal abscesses are common in proctology. Incidence is estimated at 16–28 cases per 100,000 people per year, primarily affecting young adults, with a male predominance.
In most cases, the infection originates from anal glands in the anal canal wall. These glands normally secrete mucus to ease stool passage. Obstruction can favor bacterial proliferation.
Certain conditions increase risk: inflammatory bowel disease such as Crohn’s disease, diabetes, immunosuppression, or local trauma. Anal abscesses are studied in proctology, digestive surgery, and gastroenterology.
How it works
The process usually starts with obstruction of an anal gland in the anal canal crypts. These glands normally open into the anal lumen and help lubricate stool. When debris, local inflammation, or microtrauma blocks the gland, secretions stagnate.
This stagnation creates an environment for intestinal bacteria to multiply. The most commonly involved species are Escherichia coli, Bacteroides fragilis, and other anaerobic bacteria.
Infection triggers inflammation. White blood cells migrate to fight bacteria. Part of the tissue may undergo necrosis, forming a cavity. This cavity gradually fills with pus, a mixture of bacteria, immune cells, and tissue debris.
Depending on the infection’s path in the perineal tissues, different abscess types form. Superficial abscesses remain under the skin, while deep forms spread into anatomical spaces around the rectum.
Pressure inside the abscess increases as pus accumulates, causing severe, throbbing pain. If not drained, the abscess can rupture spontaneously or create a persistent tract to the skin, forming an anal fistula.
In which cases is it used?
The term “anal abscess” is used mainly in proctology and digestive surgery to describe an acute infection requiring prompt evaluation to prevent infection spread.
Diagnosis is based on typical symptoms: sudden anal pain, localized swelling, redness, and sometimes fever. Clinical examination usually identifies superficial abscesses.
In some cases, imaging is necessary. Endoanal ultrasound, pelvic MRI, or CT scan help locate deep abscesses and detect fistulous tracts.
Management almost always involves surgical drainage, opening the abscess to remove pus and reduce tissue pressure. Antibiotics are prescribed in select cases, such as immunocompromised patients or when infection spreads.
Benefits and objectives
Treatment of an anal abscess aims to control infection and prevent complications. Medical objectives include:
✓ Rapidly evacuating the pus collection to relieve pain and reduce tissue pressure.
✓ Eliminating the bacterial source to prevent spread to neighboring structures.
✓ Preserving anal sphincter muscles during surgery to maintain continence.
✓ Identifying any associated fistulous tract, common after abscess formation.
✓ Reducing recurrence risk through complete drainage and appropriate follow-up.
Early management usually leads to quick recovery. Most patients notice significant pain relief within hours after drainage.
Risks, limitations, or controversies
Even with proper treatment, complications may occur. The most common is the development of an anal fistula, affecting approximately 30–50% of patients after an abscess if the infectious tract persists.
Deep abscesses can be challenging to diagnose because swelling may not be visible externally, necessitating imaging.
Surgical treatment has limitations. An incision that is too large or poorly placed can damage sphincter muscles, rarely causing continence problems.
Associated conditions may complicate management. In patients with Crohn’s disease, anorectal infections can be more frequent, recurrent, and difficult to treat.
Research and innovations
Research on anal abscesses focuses on fistula prevention and surgical technique improvement. MRI has significantly enhanced mapping of deep anorectal infections and fistulous tracts.
More conservative surgical techniques aim to preserve sphincter function while treating infection.
In Crohn’s disease, biologics targeting inflammatory pathways, such as anti-TNF agents, have reduced perineal complications.
Microbiological research explores the role of gut flora in abscess formation and progression to fistula, potentially improving prevention and treatment strategies.
Short FAQ
What causes an anal abscess?
The main cause is infection of an anal gland. When the gland’s duct is blocked, intestinal bacteria multiply in surrounding tissues, causing inflammation and a pus-filled cavity around the anus.
What are the first symptoms of an anal abscess?
Severe anal pain is the most common sign, often with swelling, redness near the anus, and sometimes fever. Pain usually worsens when sitting or during defecation.
Can an anal abscess heal on its own?
Spontaneous healing is rare. Without drainage, the infection often persists or worsens. Spontaneous rupture may occur but does not always treat the infection source and can lead to fistula formation.
Does treatment always require surgery?
In most cases, yes. Surgical drainage evacuates pus and quickly reduces pain. Antibiotics alone usually cannot eliminate the purulent collection.
How long does recovery take?
Pain often decreases within days after drainage. Complete wound healing can take several weeks depending on the abscess’s size and depth.
Is an anal abscess dangerous?
Most abscesses heal well with proper treatment. Untreated infection can spread to nearby tissues or cause complications such as anal fistula.
What is the difference between an anal abscess and an anal fistula?
An abscess is an acute pus-filled infection. A fistula is an abnormal channel connecting the anal canal to the skin, often appearing after abscess healing when the infectious tract persists.
Can an anal abscess be prevented?
There is no specific prevention in most cases. Good local hygiene and managing inflammatory bowel disease may reduce some risk factors.
Are anal abscesses common?
Yes. They are among the most common proctologic emergencies, with men more often affected than women.
Can abscesses recur?
Yes. Recurrence can occur if the infection source persists or a fistula develops. Medical follow-up identifies and treats these situations.
Key points
An anal abscess is an acute infection of tissues around the anus, usually due to obstruction and infection of an anal gland. It causes severe pain, localized swelling, and sometimes fever. Treatment mainly involves surgical drainage of pus. The most common complication is an anal fistula, which may develop after abscess healing. Prompt care limits infection spread and promotes complete recovery.
Related Longevity Concepts
Scientific context
Field: Clinical medicine, biology, and preventive health
Biological process: Human physiology, pathology, and health-related mechanisms
Related systems: Metabolic, immune, cardiovascular, nervous, and cellular systems
Relevance to longevity: Understanding medical terminology and biological processes helps clarify how diseases, symptoms, biomarkers, and treatments influence long-term health, prevention, and healthy aging.